Health Policy in Trump's Second Term: What Changed in Year One
How the OBBBA, Medicaid cuts, and executive orders are reshaping coverage, costs, and public health administration.
By Holly AbramsonReviewed by PAP Editoral TeamUpdated July 9, 202625+ min read
What you’ll learn in this article…
The One Big Beautiful Bill Act cuts roughly $900 billion in federal Medicaid funding over ten years, leaving 7.5 million more Americans uninsured.
Research from Georgia and Arkansas confirms Medicaid work reporting requirements failed to increase employment yet drove coverage losses.
ACA marketplace enrollment is projected to drop by 2.1 million as enhanced premium subsidies expired at the end of 2025.
The U.S. completed its withdrawal from the World Health Organization on January 22, 2026, ending nearly eight decades of membership.
Expansion versus contraction: the first year of President Trump's second term moved federal health policy decisively toward the latter. Since the January 20, 2025 inauguration, executive action and the One Big Beautiful Bill Act (signed July 4, 2025) have set in motion roughly $900 billion in Medicaid cuts over the next decade, with Congressional Budget Office projections of 7.5 million more uninsured Americans and a 2.1 million drop in ACA Marketplace enrollment.1
The practical tension for public administrators is structural. Federal retrenchment shifts fiscal and operational burdens onto states already managing 75 million Medicaid enrollees and 24 million Marketplace participants, while work reporting mandates, subsidy expirations, and civil rights rule rewrites compound the implementation load. One year in, the policy direction is no longer ambiguous: the federal share is shrinking, and state capacity is the binding constraint.
The Health Policy Landscape After One Year: A Timeline of Major Actions
In concrete terms, the first year of Trump's second term represents the most consequential restructuring of federal health programs in a generation. Within twelve months, the administration used two parallel levers, executive orders and sweeping legislation, to reshape coverage for roughly 168 million Americans enrolled in Medicaid, Medicare, and ACA Marketplace plans.
Setting the Baseline
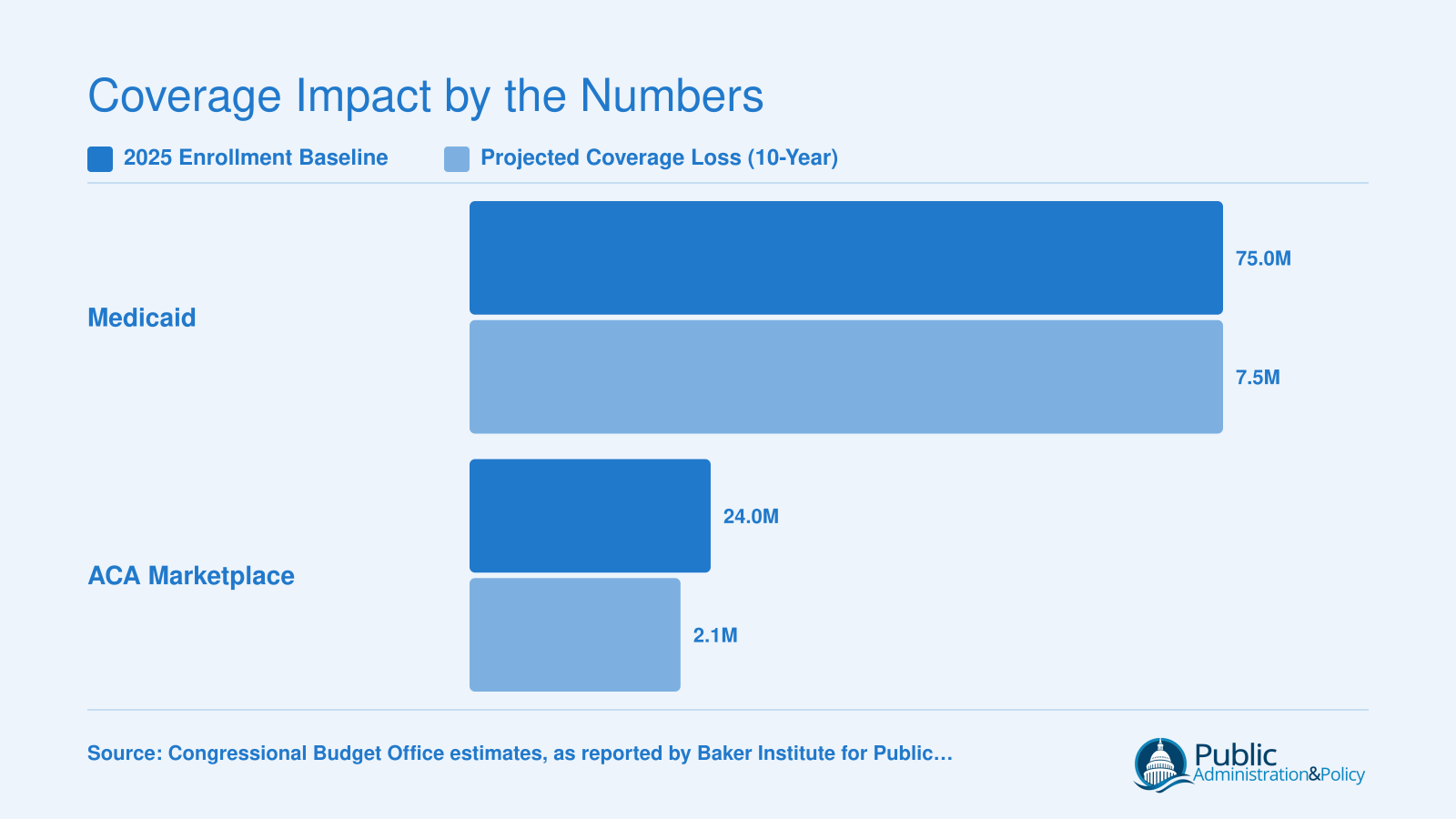
As of early 2025, the scale of the programs at stake was enormous. Approximately 75 million Americans were enrolled in Medicaid, 69 million in Medicare, and more than 24 million carried ACA Marketplace plans.1 These are not abstract statistics. They represent the population directly exposed to the policy changes that followed. For public administrators and policy analysts, this baseline is the starting point for any honest impact assessment. The Baker Institute's May 2026 review, authored by Elena M. Marks and colleagues, anchors much of the analysis in this article.1
The First Months: Executive Orders as the Opening Move
Trump was inaugurated on January 20, 2025, and the administration moved quickly.1 Where the first term relied heavily on regulatory delay and administrative friction to erode ACA implementation, the second term opened with direct executive orders targeting program administration, enrollment verification, and agency priorities. These early orders signaled the direction of travel before Congress had passed a single bill.
This dual-track strategy, using executive authority for immediate regulatory changes while simultaneously advancing legislation through Congress, gave the administration both speed and structural reach. The approach proved far more effective than the failed ACA repeal push of 2017, which collapsed in the Senate after months of negotiations.
The Pivot Point: OBBBA Signed on July 4, 2025
The legislative centerpiece arrived when Trump signed the One Big Beautiful Bill Act on July 4, 2025.1 The timing was deliberate. The OBBBA bundled Medicaid restructuring, ACA subsidy changes, and fiscal provisions into a single omnibus package, bypassing the procedural vulnerabilities that derailed repeal efforts eight years earlier. The Congressional Budget Office estimated the law would cut approximately $900 billion from Medicaid over the next decade.1
From Passage to Implementation: Mid-2025 Through Mid-2026
The period between the OBBBA's signing and mid-2026 shifted the burden of action to states. Federal agencies began issuing guidance on work reporting requirements, eligibility redetermination timelines, and changes to how states finance their Medicaid programs. For aspiring government program managers, the challenge of translating these mandates into operational reality is a defining case study in intergovernmental administration. These regulatory changes compounded the legislative cuts, creating an implementation environment that state health agencies are still navigating as of June 2026. The cumulative effect, across executive orders, statutory change, and agency rulemaking, is what makes this first year distinct in scope and speed from anything the administration attempted in its first term.
The One Big Beautiful Bill Act: How $900 Billion in Medicaid Cuts Work
The signing of the One Big Beautiful Bill Act on July 4, 2025 marked the largest successful reduction in Medicaid spending in the program's 60-year history, fundamentally restructuring how the federal government shares healthcare costs with states. Where previous retrenchment attempts fell short, including the failed ACA repeal efforts of 2017 and various per-capita cap proposals, the OBBBA succeeded by packaging Medicaid cuts within a broader reconciliation bill that linked fiscal priorities across multiple policy areas.
The Four Pillars of $900 Billion in Cuts
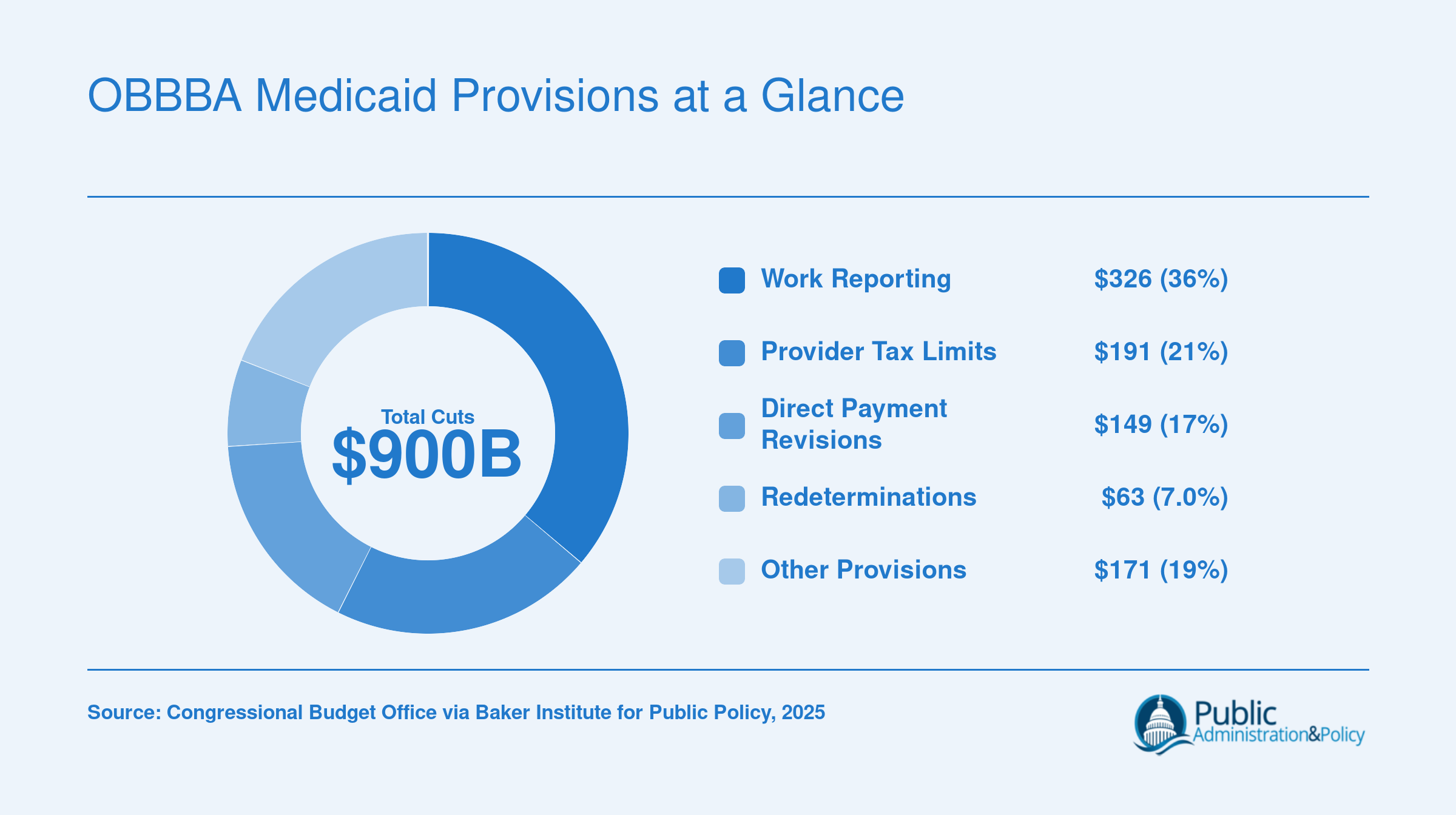
The Congressional Budget Office estimates that OBBBA will reduce federal Medicaid spending by approximately $698 billion through 2034, with total health program cuts exceeding $1 trillion when related provisions are included.1 Four primary mechanisms drive these reductions:
Mandatory work reporting requirements ($326 billion): The largest single cut requires Medicaid expansion enrollees to document work, job training, or community service hours. States must build new verification systems and manage compliance paperwork for millions of beneficiaries.
Limits on state provider taxes ($191 billion): States have long used provider taxes to draw down additional federal matching funds. New caps restrict this financing strategy, forcing states to either absorb lost revenue or reduce provider payments.2
Revisions to state direct payment programs ($149 billion): Changes to supplemental payment arrangements reduce flexibility states previously had in directing Medicaid dollars to safety-net hospitals and other providers.
Increased eligibility redeterminations ($63 billion): More frequent income and eligibility checks create administrative churn that historically results in eligible beneficiaries losing coverage during paperwork gaps.
Coverage Losses at Scale
The coverage impact of these provisions is substantial. CBO projects 7.6 million more uninsured Americans by 2034 due to Medicaid changes alone, with Medicaid enrollment declining by 10.3 million.3 When combined with the expiration of enhanced ACA marketplace subsidies, total coverage losses could reach 11.8 million people.2 Independent analyses from the Urban Institute and Commonwealth Fund suggest these estimates may be conservative, with some projections showing Medicaid enrollment losses as high as 14.4 million under certain implementation scenarios.3
The State-Level Administrative Burden
For public administration vs public policy professionals, the core concern is how OBBBA shifts both costs and administrative complexity from federal to state governments. States now face a structural dilemma: absorb significant budget shortfalls, reduce benefits or eligibility, or cut provider payments in ways that threaten healthcare infrastructure.
The downstream effects are already visible. Modeling research indicates 101 rural hospitals face high risk of closure by 2034 under these provisions.3 Federally Qualified Health Centers, which serve as primary care providers for underserved communities, project losing 5 million Medicaid patients and an 18.7 percent reduction in revenue.3 Economic analyses estimate 302,000 job losses and $135.3 billion in reduced economic output by 2034, concentrated in healthcare sectors that anchor many local economies. Those interested in the broader landscape of public administration jobs should recognize that these workforce impacts extend well beyond clinical roles.
The OBBBA represents more than a budget line item. It is a fundamental rebalancing of intergovernmental responsibilities that will test state administrative capacity for years to come.
OBBBA Medicaid Provisions at a Glance
The Congressional Budget Office estimates the One Big Beautiful Bill Act will reduce federal Medicaid funding by roughly $900 billion over the next decade. These cuts are projected to leave 7.5 million fewer Americans enrolled in Medicaid and 2.1 million fewer in ACA Marketplace plans, a combined coverage loss of 9.6 million people.
How States Are Absorbing the Fiscal Shock of OBBBA
The One Big Beautiful Bill Act has forced state governments to absorb significant fiscal shocks through multiple channels, creating immediate budgetary and administrative pressures that demonstrate classic intergovernmental tensions. Federal policy choices have translated into unfunded operational mandates for state health agencies, challenging long-standing financing mechanisms and forcing difficult tradeoffs between coverage and compliance.
Provider Tax Restrictions Disrupt State Financing Models
The $191 billion cut targeting state provider taxes strikes at a fundamental revenue mechanism that Medicaid expansion states have relied upon for decades. States like Arizona have used provider taxes and assessments to generate nonfederal match dollars, which in turn draw down federal matching funds at rates that historically ranged from 1:1 to 9:1 depending on the state's Federal Medical Assistance Percentage.1 Under OBBBA, new or increased provider taxes are prohibited starting in 2026, and the safe harbor threshold for existing taxes begins phasing down in fiscal year 2028.2 This restriction forces states to either replace those funds with general revenue, cut services, or reduce eligibility. For states where provider taxes represent a double-digit share of the nonfederal match, the budget hole can reach hundreds of millions of dollars annually, complicating legislative sessions and forcing agencies to plan for leaner operations.
Administrative Bottlenecks from Faster Redeterminations
The OBBBA mandates that Medicaid expansion enrollees undergo eligibility redetermination at least every six months, a significant acceleration from the typical twelve-month cycle. States face a December 2026 compliance deadline, meaning agencies must double their processing capacity within months.3 The Urban Institute estimates this change alone could reduce Medicaid expansion enrollment by roughly 20 percent, not because individuals lose eligibility but because shorter cycles create procedural churn: notices get lost, paperwork deadlines pass, and caseworkers struggle to keep pace.4 State human services departments are scrambling to hire and train eligibility workers, upgrade legacy IT systems to handle the volume, and manage call centers flooded with questions. These are classic public policy making challenges where policy design at the federal level creates operational friction at the state level, and states bear the cost.
State Responses Range from Compliance to Litigation
States are pursuing varied strategies. Some are seeking Section 1115 waivers to negotiate partial deferrals or alternative compliance pathways, pushing implementation timelines out to December 2028.5 Arkansas, which previously implemented and then saw its work requirement struck down in court, is proceeding cautiously, wary of repeating past administrative failures.6 Other states are restructuring their Medicaid agencies, consolidating eligibility functions, and investing in automated systems during 2026 to handle the new workload. A few have filed lawsuits challenging the constitutionality of the provider tax restrictions or the expedited redetermination mandates, arguing they violate principles of cooperative federalism. The Centers for Medicare & Medicaid Services released an implementation roadmap on April 18, 2026, but it left key details about work requirement regulations undefined, leaving states in a holding pattern.7
The Intergovernmental Relations Challenge
From a public administration perspective, OBBBA exemplifies how federal deficit reduction can externalize costs onto state bureaucracies. States did not vote for these changes, yet they must staff the call centers, defend the lawsuits, and manage the political fallout when constituents lose coverage. The law offers states no new administrative funding, turning coverage reductions into a de facto budget balancing tool. For MPA and MPP professionals, including those pursuing a health policy masters, this case study illustrates the limits of federal mandates when state capacity and political will diverge, and the importance of implementation design in determining whether policy achieves its stated goals or simply shifts burdens across levels of government.
Questions to Ask Yourself
What share of your state's budget currently depends on federal Medicaid matching funds?
Many states rely on federal matching rates between 50 and 75 percent to sustain their Medicaid programs. A $900 billion federal pullback over ten years will force governors and legislatures to choose between raising state taxes, cutting benefits, or dropping enrollment eligibility thresholds entirely.
If your agency had to redetermine eligibility for every Medicaid expansion enrollee, what staffing and IT infrastructure would you need?
OBBBA mandates increased eligibility redeterminations for millions of expansion adults. States without modern integrated eligibility systems will face cascading administrative costs, hiring freezes elsewhere, and high procedural disenrollment rates that strip coverage from people who remain eligible but miss paperwork deadlines.
How would provider tax limits change hospital financing in rural versus urban areas of your state?
Many states use provider taxes to draw down federal Medicaid dollars and fund safety net hospitals. The $191 billion cap on these taxes will hit rural hospitals hardest, where narrow margins and fewer private payers leave little room to absorb lost federal revenue or compensate for uncompensated care increases.
ACA Marketplace Changes: Subsidies, Enrollment, and What Consumers Pay Now
The expiration of the American Rescue Plan's enhanced premium subsidies at the end of 2025 is poised to drive historic increases in what consumers pay for ACA marketplace coverage, reversing years of record affordability.
The Expiration of Enhanced Subsidies and Return of the Subsidy Cliff
With no extension in the One Big Beautiful Bill Act, the enhanced subsidies that had lowered premiums for millions of households expired on December 31, 2025.12 The result is a return to the pre-2021 subsidy structure, where assistance phases out completely at 400% of the federal poverty level (FPL). That cliff means a single adult earning more than $62,600 or a family of four above $128,600 receives no financial help for marketplace plans.
For those at the edge, the jump is severe. A 60-year-old couple with an income just above 402% FPL faces an annual premium of $22,600 in 2026. An estimated 725,000 people with incomes between 400% and 500% FPL lose subsidies entirely, facing an average premium increase of $2,900 per year.4
Enrollment Impact: A Forecasted Decline of 2.1 Million
In 2025, a record 24.3 million people selected an ACA marketplace plan, and 92% of them received premium subsidies.4 The Congressional Budget Office now projects that defining public policy around subsidy eligibility will reduce marketplace enrollment by 2.1 million over the next decade.4 Most of these losses will concentrate among middle-income households that can no longer afford coverage without enhanced tax credits.
Also contributing to the decline are administrative shifts that make enrolling harder. Shortened open enrollment periods and cuts to navigator and outreach funding mean less assistance is available precisely when consumers need it most to understand their new costs.
Consumer Premium Increases Across Income Levels
Without the enhanced subsidies, marketplace premiums rise sharply for nearly all enrollees. Across the market, the average consumer premium increase for 2026 is estimated at 114%, translating to $1,016 more per year.5 Insurers proposed an 18% increase in plan costs for the year, reflecting both the policy change and underlying medical cost trends.4
For a family at 200% FPL, the subsidies previously capped premiums at about 2% of household income. That cap now disappears, leaving families exposed to much higher out-of-pocket costs. At 300% FPL, the prior cap of approximately 6% of income also vanishes, meaning a family could see premiums double or triple relative to what they paid in 2025. These sharp increases will force many to reassess whether keeping coverage is financially feasible.
Comparing Policy Trajectories: Biden-Era Expansion Vs. Trump Second-Term Contraction
Understanding how federal health policy shifted between administrations requires examining specific policy levers side by side. The table below compares six dimensions where the Biden and Trump second-term approaches diverged most sharply. For policy professionals and MPA/MPP students, this comparison illustrates how changes in federal posture create cascading effects on state budgets, enrollment systems, and coverage outcomes. Data points draw on Congressional Budget Office estimates and published enrollment figures; where precise figures are not yet available, directional trends are noted.
Policy Dimension
Biden Administration (2021 to 2025)
Trump Second Term (2025 to 2026)
Medicaid Enrollment Direction
Expanded coverage through enhanced federal matching rates and continuous enrollment requirements during the public health emergency; approximately 75 million enrollees by early 2025
OBBBA provisions projected to reduce Medicaid enrollment by 7.5 million over the next decade through eligibility redeterminations, work reporting mandates, and funding restructuring
ACA Marketplace Subsidies
Extended and enhanced premium tax credits under the Inflation Reduction Act, reducing out-of-pocket costs for millions of enrollees
Allowed enhanced subsidies to expire; OBBBA did not renew expanded premium assistance, increasing consumer costs for an estimated 2.1 million who may lose Marketplace coverage
Enrollment Outreach and Navigator Funding
Restored and increased funding for ACA enrollment navigators and outreach campaigns to maximize sign-ups
Reduced federal investment in enrollment outreach, shifting responsibility to states and private entities
Medicaid Work Reporting Requirements
Did not pursue federal work requirements; rescinded prior waivers that conditioned Medicaid eligibility on employment verification
Mandated work reporting for Medicaid expansion enrollees, a provision CBO estimates will account for roughly $326 billion in Medicaid savings over ten years. Research from Georgia and Arkansas found no significant increase in workforce participation under similar requirements
State Provider Tax Treatment
Maintained existing rules allowing states to levy provider taxes to draw down federal Medicaid matching funds
OBBBA limits state provider tax mechanisms, projected to reduce state Medicaid financing capacity by approximately $191 billion over the next decade
Net Coverage Trajectory
Coverage gains: uninsured rate reached historic lows by 2023, driven by Marketplace enrollment exceeding 24 million and sustained Medicaid rolls
Coverage contraction: combined Medicaid and Marketplace losses projected at roughly 9.6 million over the coming decade, reversing prior coverage gains
Medicaid Work Reporting Requirements: What the Evidence Actually Shows
Work reporting requirements for Medicaid have moved from a contested state waiver experiment to federal law, and the evidence base built over the past seven years is now colliding with national implementation. The OBBBA requires states to verify that adult expansion enrollees are working, in school, caregiving, or formally exempt, with reporting at intervals tight enough that most state Medicaid agencies are now scrambling to build or procure verification systems before deadlines hit.
How the Federal Mandate Differs from Earlier State Waivers
Arkansas (2018-2019) and Georgia's Pathways to Coverage (launched 2023) were limited, opt-in state experiments under Section 1115 waivers.5 The OBBBA flips that posture: work reporting is now a condition of federal Medicaid expansion dollars, applied uniformly across all expansion states, with verification frequency and exemption categories defined in statute rather than negotiated waiver-by-waiver.4 States lose flexibility on whether to participate but gain full responsibility for the administrative apparatus.
What the Evidence Says About Employment
The Arkansas rollout produced no significant increase in employment among affected enrollees, according to follow-up research, while disenrollment correlated strongly with practical barriers like lack of internet access rather than unwillingness to work.2 Georgia's enrollment has run well below what traditional expansion would have produced.5 CBO scored the employment effect of the national mandate as negligible.2 The underlying reason is structural: roughly 64% of Medicaid adults are already working, another 12% are caregivers, 10% are disabled, and 7% are in school. Only about 8% are not working and not in an exempt category, and most of that group cycles in and out of low-wage jobs that already qualify.2
Administrative Burden and the Source of the Savings
The $326 billion in projected Medicaid savings tied to work reporting does not come from enrollees moving to employer-sponsored coverage. It comes from coverage losses. Microsimulation work and analyses from the Urban Institute, Commonwealth Fund, and Kaiser Family Foundation converge on a projected coverage loss of 5.5 to 6.3 million people in 2026 alone, rising toward 10.3 million by 2034.31 A consistent finding across these models: most of the people who lose coverage are working, seeking work, or qualify for an exemption but fail to document it in time.1
For state administrators, the implication is concrete. Verification platforms, call center capacity, exemption adjudication, and appeals processing all cost money, and federal funding to expansion states is projected to drop by $33 to $46 billion in 2026.2 Professionals pursuing MPA in finance and budgeting credentials will find these intergovernmental fiscal pressures increasingly central to their work. The policy design tension is sharp: states are being asked to spend more on administration to enforce a requirement that the evidence suggests will not move employment, while absorbing the political and budgetary fallout of churn-driven coverage losses that fall disproportionately on Black enrollees and people with disabilities.2
Research from Georgia and Arkansas found that Medicaid work reporting requirements produced no meaningful increase in employment. The $326 billion in projected savings attributed to these mandates comes almost entirely from eligible people losing coverage due to paperwork and compliance barriers, not from enrollees moving into the workforce.
Reproductive Health, Gender-Affirming Care, and Civil Rights Rollbacks
Health policy in the second Trump administration has moved well beyond coverage and financing. A parallel track of executive actions, regulatory rewrites, and enforcement shifts has reshaped the federal posture on reproductive health, gender-affirming care, and civil rights protections inside the health system. For public administrators, the operational question is no longer just what the rules say, but how state agencies, providers, and grantees reconcile conflicting federal and state mandates.
A Post-Dobbs Abortion Policy with Federal Reach
In the first term, abortion policy operated against the backdrop of Roe. In the second term, federal action lands in a fragmented legal environment where states set their own baselines, which magnifies the effect of every federal lever.
Mexico City Policy: Reinstated and expanded early in 2025, the policy again bars U.S. global health assistance to foreign NGOs that provide or counsel on abortion, with a broader scope than prior versions.
Hyde Amendment enforcement: The administration has tightened guidance interpreting Hyde across HHS programs, narrowing the circumstances in which federal dollars may touch abortion-related services.
Title X and grant conditions: Family planning grantees face revised conditions that affect referral practices and the separation of funding streams.
States that built reproductive health infrastructure after Dobbs, including funding clinics, travel support, and Medicaid coverage of abortion using state-only dollars, now navigate federal funding conflicts that complicate cost allocation, audits, and program administration. Professionals in grant administration are on the front lines of parsing these new requirements.
Gender-Affirming Care and Civil Rights Rollbacks
The administration has rolled back the Biden-era Section 1557 nondiscrimination rule under the ACA, removing explicit protections against discrimination based on gender identity in federally funded health programs. Title IX guidance has been revised in ways that flow into school-based health services and university health plans. Enforcement of the Freedom of Access to Clinic Entrances (FACE) Act has been narrowed, with the Justice Department deprioritizing prosecutions and pardoning prior offenders.
Implications for State Administrators
For state health agencies, the practical work is reconciling federal rules with state statutes that may run in the opposite direction. That means rewriting provider contracts, updating Medicaid manuals, retraining eligibility staff, and preparing for litigation risk on multiple fronts at once. Understanding the importance of public policy frameworks is essential for administrators who must translate these shifting mandates into day-to-day operations.
Public Health Infrastructure: WHO Withdrawal, Agency Shakeups, and Pandemic Readiness
On January 22, 2026, the United States completed its withdrawal from the World Health Organization, severing a relationship that had lasted nearly eight decades.1 The move, initiated by Executive Order 14155 on President Trump's first day back in office, left hundreds of millions of dollars in unpaid dues and withdrew all U.S. personnel from WHO engagements worldwide.2 The WHO, in a formal statement, expressed regret over the departure, while the Infectious Diseases Society of America characterized it as a "shortsighted and misguided abandonment of global health commitments."3
The Mechanics of the Withdrawal
The withdrawal process, which took the full one-year period required under U.S. law, terminated American participation in hundreds of WHO-led initiatives.4 As of early 2026, the U.S. no longer contributes to the Global Influenza Surveillance and Response System, a network critical for identifying emerging flu strains and selecting annual vaccine compositions. The IDSA warned that the absence "severely hampers vaccine strain selection," leaving both domestic and global health authorities with diminished data on circulating pathogens.3 U.S. personnel were recalled from all WHO technical engagements, and the government halted funding for collaborative surveillance programs that previously relied on American financial and scientific resources.
Consequences for Global Surveillance and Vaccine Development
Without U.S. participation in WHO-coordinated surveillance, the bilateral arrangements the administration has pursued to replace multilateral cooperation face skepticism from infectious disease experts. The CDC, NIH, and FDA have been instructed to continue leadership through bilateral engagements, but the loss of real-time data sharing within the WHO network creates blind spots in early warning systems for novel pathogens.4 Outside assessments describe this shift as an undermining of collective readiness, with the United Nations warning that the withdrawal "makes the world less safe."5 Gaps in influenza tracking alone could delay vaccine updates, potentially increasing the burden of seasonal and pandemic influenza domestically.
Domestic Agency Realignments and Bilateral Efforts
The CDC, NIH, and FDA have not experienced wholesale budget eliminations tied directly to the WHO withdrawal, but their international administration missions have been reoriented. Rather than contributing to shared global surveillance, these agencies now operate through a patchwork of country-specific agreements, which lack the standardized data platforms the WHO provided. Public health attorneys and policy analysts note that bilateral work cannot replace the multilateral consensus-building needed for rapid response during health emergencies. At the state and local level, health departments that previously relied on WHO-informed guidance now face fragmented information flows, complicating preparedness planning.
Mental Health and Substance Use Programs: No Direct Hit, but Context Matters
As of mid-2026, no direct changes to the Substance Abuse and Mental Health Services Administration (SAMHSA), opioid response initiatives, or the 988 Suicide & Crisis Lifeline have been documented as a result of the WHO withdrawal.4 Funding and programmatic support for these domestic mental health and substance use services remain in place under existing appropriations. However, the broader restructuring of federal public health agencies, including potential leadership changes and reprioritization of resources, creates an environment of uncertainty for long-term behavioral health investments. While 988 call centers continue to operate and opioid settlement funds flow separately, the withdrawal signals a narrower federal commitment to global health governance, which could eventually influence the perceived legitimacy of domestic public health infrastructure.
Coverage Impact by the Numbers
The One Big Beautiful Bill Act and related administrative changes are projected to reduce health coverage for nearly 10 million Americans over the next decade. The scale of these losses becomes clearer when measured against the enrollment baselines that existed in 2025, before the law took effect.
What This Means for Public Policy Careers and MPA/MPP Students
What kinds of public sector jobs will be in highest demand as states absorb OBBBA's Medicaid changes through 2030? The short answer: roles that sit at the intersection of program administration, finance, and federal-state negotiation. The year-one record of the second Trump administration has reshaped where the hiring pressure lands and which technical skills employers are screening for.
Where the Hiring Pressure Is Landing
State health and human services agencies are the front line. With mandatory work reporting for Medicaid expansion enrollees, more frequent eligibility redeterminations, and restructured provider tax arrangements, states need administrators who can stand up new verification systems, manage call center surges, and document compliance for CMS. Counties running enrollment operations are similarly stretched. Expect openings for Medicaid program managers, eligibility operations leads, and IT-adjacent policy staff who can translate statute into workable case management workflows. Those drawn to oversight roles should explore the path to becoming a government program manager, a position increasingly critical in states navigating these federal mandates.
Specializations Gaining Relevance
Four areas have moved from useful to central for MPA and MPP graduates:
Health policy analysis: modeling coverage losses, premium effects, and uncompensated care impacts at the state level.
Intergovernmental relations: negotiating waivers, managing CMS correspondence, and coordinating with legislatures on state share funding.
Healthcare finance: restructuring provider tax arrangements, directed payment programs, and hospital reimbursement under tighter federal match rules.
Public health emergency management: rebuilding readiness capacity as federal agencies contract and WHO ties loosen.
Where Federal-State Friction Creates Opportunity
Disagreement between Washington and statehouses is itself a job creator. Legislative budget offices, state auditors, governors' policy shops, and nonpartisan research arms (MACPAC, state-level equivalents, university policy centers) all need analysts who can quantify what a federal pullback costs a specific state. Program evaluators with quasi-experimental training are particularly valued for work requirement assessments, given how thin the existing evidence base is. The breadth of careers in public administration continues to expand as these fiscal pressures intensify.
Health Policy Literacy as a Differentiator
For students currently in MPA or MPP programs, treat health policy literacy as a portable credential. Even graduates aiming for transportation, education, or housing roles will encounter Medicaid's fiscal shadow, since state budgets are increasingly defined by what health spending leaves behind. Coursework in health economics, a capstone tied to a state Medicaid agency, or a summer placement with a hospital association will read clearly on a resume in this hiring climate. Developing strong leadership skills for healthcare administrators can further distinguish candidates in a competitive job market shaped by ongoing policy upheaval.
Frequently Asked Questions About Trump's Second-Term Health Policies
The health policy changes enacted during the first year of Trump's second term have raised urgent questions for consumers, state administrators, and policy professionals alike. Below are answers to the most common questions, grounded in Congressional Budget Office projections and peer-reviewed research.
How will Trump's second-term health policies affect my insurance coverage?
The combined effects of the One Big Beautiful Bill Act (OBBBA) and administrative changes to the ACA Marketplace are projected to leave roughly 9.6 million more Americans without coverage over the next decade: 7.5 million through Medicaid reductions and 2.1 million through Marketplace enrollment declines. If you currently receive Medicaid through expansion eligibility or rely on enhanced ACA subsidies, your coverage is most directly at risk.
What is the One Big Beautiful Bill Act and how does it change Medicaid?
Signed on July 4, 2025, the OBBBA restructures Medicaid financing by cutting an estimated $900 billion over ten years. Major provisions include mandatory work reporting requirements for expansion enrollees (saving $326 billion federally), caps on state provider taxes ($191 billion), revisions to direct payment programs ($149 billion), and more frequent eligibility redeterminations ($63 billion). Together, these measures shift significant fiscal and administrative burdens to states.
What happens to Obamacare subsidies under Trump's second term?
Enhanced ACA Marketplace premium subsidies, originally expanded during the Biden administration, were not renewed under current policy. With over 24 million Americans enrolled in Marketplace plans as of 2025, the expiration of these subsidies is expected to raise out-of-pocket costs for many enrollees and reduce total Marketplace enrollment by approximately 2.1 million people over the coming decade.
Do Medicaid work requirements actually increase employment?
Research suggests they do not. Studies of Medicaid work reporting mandates in Georgia and Arkansas found no significant increase in workforce participation among affected populations. Instead, these requirements primarily function as administrative barriers that cause eligible individuals to lose coverage due to paperwork burdens and reporting confusion, rather than motivating new employment.
How does Trump's second-term abortion policy differ from his first term?
While the first term focused on appointing Supreme Court justices who ultimately overturned Roe v. Wade, the second term has moved toward using executive authority and federal funding mechanisms to further restrict reproductive health access. Federal agencies have tightened rules around Title X family planning grants, and proposed regulations limit the scope of gender-affirming and reproductive care covered by federally funded programs.
What are the effects of the U.S. withdrawing from the WHO?
Withdrawing from the World Health Organization reduces American influence over global disease surveillance, pandemic preparedness coordination, and international health standards. It also disrupts funding for programs addressing infectious disease outbreaks in lower-income nations. For domestic public health, the withdrawal limits access to real-time global epidemiological data that federal and state agencies rely on for early warning and response planning.
Health policy in 2026 is, at its core, a story about who pays and who administers when Washington steps back. The One Big Beautiful Bill Act locks in roughly $900 billion in Medicaid reductions over ten years, but the political and operational choices that determine whether 7.5 million people actually lose coverage will be made in state capitols, not Congress.
Why 2027 Matters More Than 2026
Most OBBBA provisions phase in through 2027 and beyond, meaning year one was preparation; the next several years are implementation. Track state legislative sessions, waiver applications, and eligibility redetermination data as the real measure of impact.
For MPA and MPP readers weighing specializations, health policy concentrations and state-level Medicaid, budget, and health agency roles are where the consequential work now sits. Understanding the broader landscape of importance of policy making will help graduates connect these structural shifts to the career opportunities emerging across every level of government.