The FDA's CNPV Pilot Program: What Public Administrators Need to Know
How a new voucher-based review model is reshaping federal drug approval — and what it means for regulatory policy design.
By Holly AbramsonReviewed by PAP Editoral TeamUpdated June 24, 202625+ min read
What you’ll learn in this article…
The CNPV pilot, launched June 2025, shrinks FDA review times to just one to two months.
Seven approvals as of May 2026 include a first gene therapy for genetic hearing loss.
Nontransferable vouchers prevent the accelerated review benefit from being sold for hundreds of millions.
Safety and efficacy standards remain unchanged; speed comes from parallel review, not shortcuts.
The FDA can now complete a priority drug review in as few as one to two months, far faster than the six-plus months a standard priority designation requires. That acceleration drives the Commissioner's National Priority Voucher (CNPV) pilot, a regulatory experiment testing whether intensive, parallel review can deliver speed without compromising safety or efficacy.
For MPA and MPP professionals, the CNPV is a live case study in redesigning review pathways, integrating cross-cutting councils, and targeting national priorities, design choices with lessons for public policy making across government.
Early approvals have shown potential to boost domestic manufacturing resilience and address unmet medical needs, but questions about resource strain, post-market monitoring, and equitable access persist.
What Is the CNPV Pilot Program?
Federal regulatory agencies are increasingly piloting adaptive review frameworks to address pressing public health needs. The FDA's Commissioner's National Priority Voucher (CNPV) Pilot Program, announced in June 2025, is one such initiative: a targeted effort to dramatically shorten review timelines for certain drugs and biologics without compromising scientific standards.
A New Kind of Priority Review
The CNPV pilot allows the FDA to grant a nontransferable voucher for a specific drug or biological product application. Once a voucher is assigned, the application enters a dedicated accelerated pathway with a target review time of just one to two months. This stands in stark contrast to the agency's standard priority review timeline, which typically takes six months or longer. The program is designed to create a faster lane for products that align with clearly defined national health priorities, but it does not create a separate approval track. All statutory and regulatory requirements for demonstrating safety and effectiveness remain in force. Speed does not mean a lower bar: the FDA must still find substantial evidence of benefit that outweighs risks before granting approval.
Preserving Rigor at Speed
A common misconception is that accelerated reviews sacrifice thoroughness. Under the CNPV pilot, the FDA applies the same statutory and regulatory approval standards that govern any drug or biologic. The agency's scientific review teams continue to evaluate clinical data, manufacturing quality, and labeling accuracy with full rigor. The difference lies in process mechanics: dedicated resources, streamlined coordination across disciplines, and early engagement with sponsors allow the FDA to compress timelines without short-circuiting the analysis. The program's design is thus a case study in how administrative efficiency can coexist with regulatory integrity, a tension at the heart of defining public policy in high-stakes domains.
Nontransferable Vouchers, a Deliberate Design
One feature that distinguishes the CNPV pilot from older FDA voucher programs is the nontransferable nature of the vouchers. Unlike the tropical disease priority review vouchers, which companies can buy and sell on a secondary market, a CNPV voucher is tied to a specific application and cannot be transferred to another product or entity. The FDA structured the pilot this way to prevent gaming and to ensure that the accelerated review is reserved for candidates that genuinely meet the program's public health criteria. This choice reflects a policy judgment that the public benefit should not be commoditized.
Scope and Authority
The CNPV pilot covers applications for drugs and biological products. When a sponsor applies, a multidisciplinary CNPV Review Council, dubbed a "tumor board-style" group, evaluates the submission. However, the council does not hold final approval authority. That responsibility rests with the FDA center that normally regulates the product, such as the Center for Drug Evaluation and Research or the Center for Biologics Evaluation and Research. This separation ensures that career scientific staff, rather than a temporary council, make the ultimate safety and effectiveness determinations. The program therefore layers a strategic prioritization mechanism on top of, not instead of, the FDA's standard review infrastructure.
The Five National Health Priorities Driving the Program
The CNPV pilot program channels FDA review resources toward five explicitly defined national health priorities, each with distinct eligibility criteria that applicants must meet to qualify for a voucher.
How Each Priority Shapes Eligibility
Public health crisis response: Covers countermeasures for biological, chemical, or radiological threats and emerging infectious diseases. Products must address a declared or anticipated emergency, such as a new antiviral for a pandemic pathogen.
Innovative breakthrough therapies: For treatments that substantially improve upon existing options for serious diseases, requiring early clinical evidence of a major advance over standard care.
Large unmet medical needs: Targets conditions with no approved therapy or where current treatments fall short, especially rare diseases; applicants must show significant unmet clinical burden.
Onshoring and supply chain resilience: Prioritizes domestic manufacturing of essential medicines. Qualification demands proof that the product will be made in the U.S. or will shore up vulnerable supply chains.
Affordability: Considers a product's potential for substantial cost savings to patients or the system, a novel element that introduces economic analysis into FDA decision-making. Example: a generic drug that undercuts a monopolist's pricing.
Policy Implications: Stretching the Regulatory Mandate and Aligning with National Goals
The inclusion of affordability as a review criterion marks a significant departure for the FDA, an agency whose legal mandate centers on safety and efficacy, not cost. This has stirred debate among policy observers: while lowering drug prices is a widely shared goal, asking the FDA to assess economic value could strain its scientific objectivity and invite litigation. At the same time, each priority reflects a deliberate effort to sync the CNPV with larger federal strategies. Crisis response builds on pandemic-era reforms, supply chain onshoring echoes the CHIPS Act and executive orders to reduce pharmaceutical import dependence, unmet needs mirror the goals of the Orphan Drug Act, and affordability nods to the drug pricing provisions of the Inflation Reduction Act. For health policy masters programs, the CNPV serves as a vivid case study in how a regulatory agency can absorb cross-cutting public policy-making mandates without explicit new legislation, and the delicate balancing act required to do so.
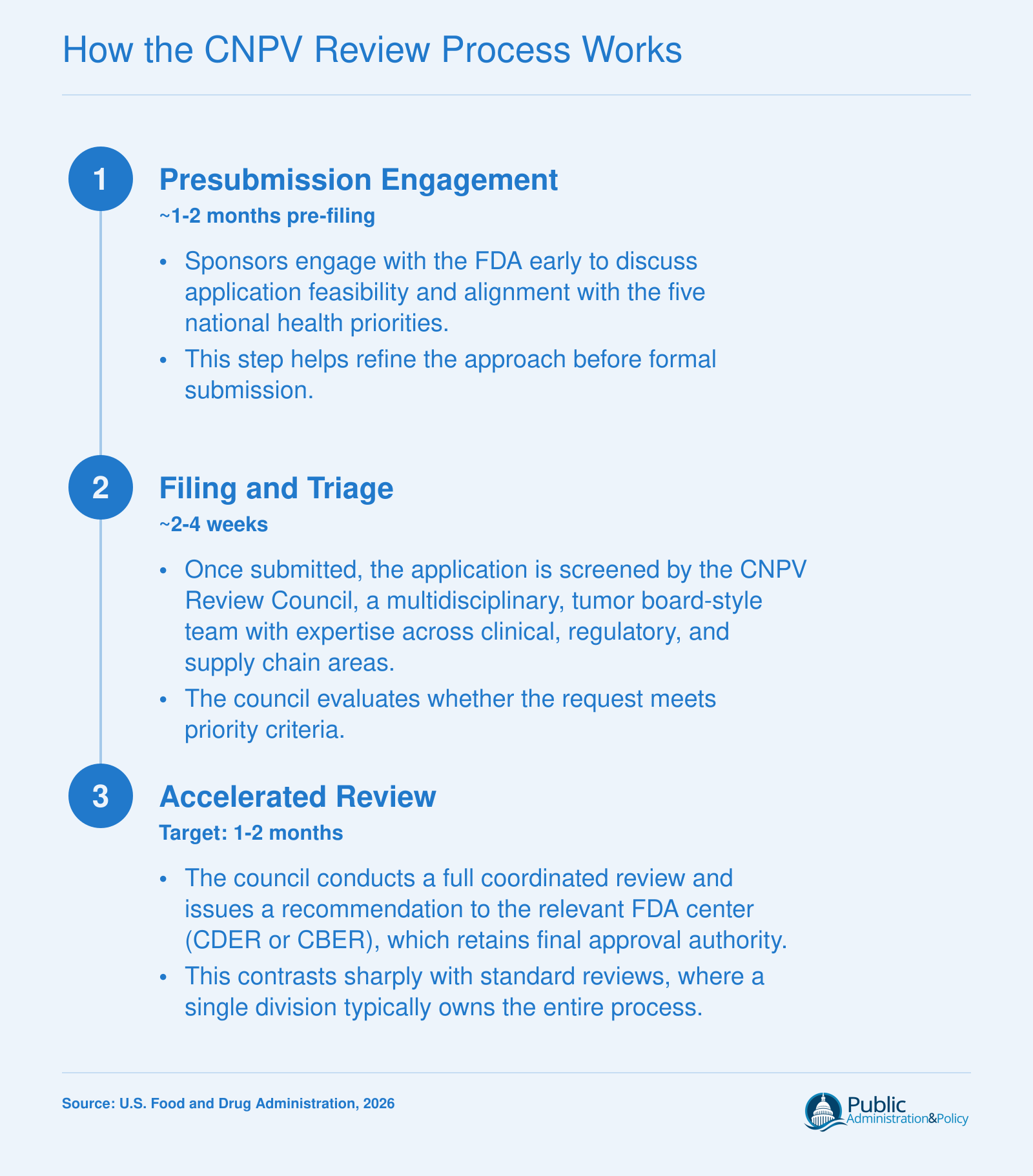
How the CNPV Review Process Works
The CNPV pilot introduces a streamlined, multidisciplinary review process that compresses timelines dramatically while preserving scientific rigor. Here is how applicants move through the program.
CNPV Approvals and Milestones Through May 2026
Which products have actually been approved through the FDA's Commissioner's National Priority Voucher pilot, and what do those approvals reveal about the program's trajectory? By May 2026, seven decisions spanning antibiotics, cancer therapies, a metabolic treatment, and a first-of-its-kind gene therapy had been made, each targeting a defined national health priority and each clearing review in a window measured in weeks rather than months.1
The First Approval: A Domestic Manufacturing Milestone
On December 9, 2025, the CNPV pilot logged its first approval for an antibiotic manufactured in the United States.1 The decision directly addressed the national priority of increasing domestic drug manufacturing, a goal that gained urgency during recent supply chain disruptions. The product's name and sponsor have not been publicly disclosed, but the approval validated the pilot's ability to move a therapy from application to market in roughly two months.
Building Momentum in Early 2026
March 2026 brought two notable additions. On March 5, the FDA approved ticlimab (sponsored by Johnson & Johnson's Janssen unit) for adults with relapsed or refractory multiple myeloma.2 Then on March 19, a higher-dose formulation of semaglutide received CNPV authorization, expanding treatment options for metabolic disease.1 These approvals demonstrated the program's reach across therapeutic areas.
Breakthroughs: First NME and Gene Therapy
April 1, 2026, saw the first new molecular entity (NME) cleared under the pilot, though details about the product remain limited.1 Just three weeks later, on April 23, the FDA approved a gene therapy for genetic hearing loss, marking a historic first for both the CNPV pathway and the field of inherited deafness treatments.1 This decision illustrated the pilot's capacity to accelerate access to transformative innovations, a point that connects directly to federal program management principles around pilot design and performance benchmarking.
May Additions and Cumulative Impact
The seventh CNPV approval arrived on May 8, 2026, for Bizengri (zenocutuzumab-zbco), sponsored by Partner Therapeutics, Inc.3 The drug targets advanced unresectable or metastatic cholangiocarcinoma in patients with an NRG1 gene fusion, addressing a rare and hard-to-treat cancer. By this point, the pilot had already awarded its first two vouchers, on December 19, 2025, and April 24, 2026, and the mix of products underscored the breadth of the five national health priorities.1
These seven decisions, while modest in number, signal that the CNPV review council can meet aggressive timelines without sacrificing the FDA's safety and effectiveness standards, a conclusion the public hearing in March 2026 reinforced.2
Questions to Ask Yourself
Could a voucher-based incentive model, nontransferable and priority-linked, work in your agency's regulatory context?
Adapting it demands clear public-priority criteria and safeguards against gaming. Assess whether your agency can tie accelerated treatment to national interest without distorting industry behavior.
What safeguards would prevent political influence from skewing which applications receive accelerated treatment?
The CNPV uses a multidisciplinary council, but final sign-off lies with centers. Consider how you would embed transparency and accountability to shield decisions from external pressure.
How would you measure whether faster review timelines compromise scientific rigor?
Speed gains must not erode safety standards. Design metrics that pair time-to-decision with post-market monitoring to detect any decline in review quality over the pilot period.
How the CNPV Compares to Other FDA Expedited Pathways
An accelerated six-month priority review can bring a promising therapy to patients months faster than a standard review, but what if that timeline could shrink to just one or two months? The CNPV pilot program deliberately compresses review time far beyond what the other expedited pathways offer, while adding a layer of collaborative evaluation that is unique in the FDA's portfolio. For public administrators, understanding where CNPV sits relative to programs like fast track, breakthrough therapy, accelerated approval, and standard priority review illuminates how regulatory innovation can target national priorities without rewriting the underlying approval framework.
A Targeted Accelerator, Not a Universal Shortcut
The CNPV pilot is distinct in both its scope and its mechanics. Unlike fast track or breakthrough therapy designation, which can apply to a wide range of serious conditions, CNPV starts with the Commissioner's identification of specific applications that align with the five national health priorities. The program does not replace or modify existing expedited pathways. Instead, it adds a parallel, more intense acceleration option for a narrow subset of products that carry strategic public value. Vouchers are nontransferable, which sets CNPV apart from the tropical disease priority review voucher system where vouchers can be sold. Once granted, the CNPV voucher compels the relevant FDA center to deliver a review timeline of approximately one to two months, substantially shorter than the six-month goal of standard priority review.
How It Stacks Up Against Other Pathways
Priority Review (standard): Reduces the review clock from ten months to six months for drugs or biologics that offer significant improvements in treatment, diagnosis, or prevention. CNPV slashes that further, but only for Commissioner-selected applications.
Fast Track: Designed to facilitate development and expedite review of drugs for serious conditions with unmet medical need. It allows rolling submission and more frequent FDA interaction, but the review timeline itself remains subject to the underlying priority or standard clock. CNPV does not alter the development phase; it exclusively accelerates the final review.
Breakthrough Therapy: Requires preliminary clinical evidence of substantial improvement over available therapy. It brings intensive FDA guidance during development but, like fast track, does not guarantee a one- to two-month review. Breakthrough-designated products often receive standard priority review, not the compressed CNPV timeline.
Accelerated Approval: Relies on surrogate endpoints to speed market entry and requires post-market confirmatory studies. CNPV, in contrast, still demands full demonstration of safety and effectiveness under standard statutory standards, the speed comes from resource allocation and process redesign, not from lowering evidence thresholds.
Overlaps and Limitations: Consult the Official Guidance
The FDA's "Guidance for Industry: Expedited Programs for Serious Conditions" explains which pathways can be combined. A product might hold fast track, breakthrough therapy, and priority review simultaneously, but CNPV selection is a separate decision made by the Commissioner with input from the CNPV Review Council. Whether a CNPV voucher can coexist with other designations depends on the specific facts and the latest policies, which are articulated in Federal Register notices and guidance updates. Because the pilot is still evolving, public administrators and policy analysts should verify current rules directly through the FDA's CNPV pilot program page, which publishes detailed comparison tables, review timelines, and frequently asked questions. Drug developers are also encouraged to consult the appropriate FDA review division for case-specific eligibility.
Why the Distinction Matters
For agencies studying how to build similar rapid-response mechanisms, the CNPV pilot demonstrates that extreme speed is achievable without changing the statutory safety or efficacy standards. The trade-off resides in resource intensity, a narrow scope, and a governance model that centralizes selection authority in the Commissioner's office. By comparing these features with those of other expedited programs, public administration professionals can better assess which levers, whether timeline compression, collaborative review, priority alignment, or voucher incentives, might transfer effectively to other regulatory environments.
At its core, the CNPV pilot demonstrates that accelerated regulatory timelines can be achieved through parallel review processes and intensive resources, rather than by lowering safety or efficacy standards. For public administrators, this distinction is critical: it proves that speed and scientific rigor are compatible goals in regulatory design, offering a template for process innovation without sacrificing public protection.
Policy Implications for Public Administration
Two paths exist to accelerate federal review: one that tightens timelines within existing silos, and another that reshapes the decision-making structure itself. The Commissioner's National Priority Voucher (CNPV) pilot program chooses the second route, coupling a cross-cutting council with an affordability demand that the FDA has never wielded before. For public administration, the pilot is more than a regulatory fast lane , it is a live experiment in collaborative governance, boundary-pushing public policy making, and institutional design under political uncertainty.
Collaborative Governance in Action
The CNPV Review Council pools experts from drug evaluation, biologics, and policy offices to assess applications in a "tumor board-style" format. This model preserves the legal authority of each FDA center to grant final approval, but it embeds multidisciplinary scrutiny earlier in the process. Public administrators should note the balancing act: the council adds a layer of coordination without rewriting statutory roles. That structure could translate to other domains , environmental permitting, grant-making, or multi-agency initiatives , where speed and scientific rigor often collide. The key is that line authority remains undisturbed, reducing bureaucratic turf wars while still injecting cross-functional insight.
Affordability as a Stealth Policy Experiment
Perhaps the most audacious element of the CNPV pilot is its inclusion of affordability among the five national priorities. The FDA has no statutory mandate to regulate drug prices2, and the program's affordability commitments are non-binding.2 At the June 4, 2026 public hearing3, testimony repeatedly underscored that the agency lacks pricing authority, and the Brookings Institution quickly flagged the need for enforceable mechanisms.2 Yet the pilot is forcing a conversation: can a health agency nudge companies toward value-based pricing through competitive access to a faster review window?4 The USC Schaeffer Center's comments called for clear rules or guidance5, while pharmaceutical advisory firms labeled the requirement controversial.6 For public administrators, the experiment reveals both the potential and the peril of extending an agency's influence into territory well outside its traditional writ.
Political Durability of Commissioner-Level Initiatives
The CNPV pilot sits on the personal authority of the FDA commissioner, not on a statutory mandate. That makes it vulnerable to leadership transitions and shifting White House priorities. What happens when a new commissioner takes office with a different view of the agency's role in affordability? Without a legislative anchor, the program could be halted, reshaped, or quietly deprioritized. Public administrators designing similar high-visibility pilots should consider embedding sunset clauses, published evaluation metrics, and multi-stakeholder advisory bodies , all of which create structural inertia that outlasts any single appointee. Trump health policy in the second administration offers a recent illustration of how quickly commissioner-level priorities can shift when executive leadership changes.
Preventing Voucher Commodification
A deliberate policy choice separates the CNPV from the tropical disease priority review voucher (PRV) system: CNPV vouchers are strictly non-transferable.1 In the PRV market, sponsors have sold vouchers for over $100 million, creating a secondary financial instrument the FDA never intended. By barring transfers, the CNPV prevents commodification and keeps the incentive tied directly to a sponsor's own product. This design choice reflects a hard-learned lesson: when a regulatory asset becomes tradable, market dynamics can distort the original policy goal. It is a useful precedent for agencies contemplating voucher-like incentives in other sectors.
Challenges, Risks, and Open Questions
The CNPV pilot is a bold regulatory experiment, but every accelerated pathway introduces new tensions. By compressing review timelines to one to two months, the program places intense demands on the FDA's scientific and administrative infrastructure. These pressures ripple beyond the pilot itself, raising questions about long-term viability, equitable access, and unintended consequences.
Strain on Reviewer Capacity and Agency Resources
Prioritizing CNPV applications inevitably diverts expert staff away from other reviews. The program's multidisciplinary "tumor board" model requires senior scientists, clinicians, and policy analysts to dedicate concentrated blocks of time to each voucher request. This comes atop an already heavy workload of standard and expedited submissions. General concerns about reviewer burnout and retention within federal regulatory agencies are well documented, and any pilot that further concentrates high-stakes decisions into compressed windows risks exacerbating those strains. While the FDA has not publicly detailed resource reallocations for the pilot, public administration researchers often note that unfunded mandates or rigid performance targets can lead agencies to shift resources internally in ways that create backlogs elsewhere. Broader questions about civil service reform are increasingly relevant as agencies face mounting pressure to deliver more with constrained budgets.
Equity Concerns in Priority Setting
The five national health priorities guiding voucher eligibility, crisis response, breakthrough innovation, unmet need, supply chain resilience, and affordability, are broadly framed. Critics from health equity organizations have raised general cautions about whether such criteria may favor well-resourced sponsors with sophisticated regulatory affairs teams. Smaller biotech firms, academic researchers, or treatments for conditions that disproportionately affect marginalized communities could face barriers navigating a compressed, invitation-style process. In academic discourse, similar expedited pathways have been questioned for potentially widening disparities if the applications that succeed tend to cluster around commercially attractive areas rather than neglected public health needs. Without careful oversight, the promise of rapid approval for priority therapies might not translate into equitable access for patients across socioeconomic and demographic lines.
Transparency and the Risk of Favoritism
Voucher awards are nontransferable and ultimately approved by the relevant FDA center, yet the CNPV Review Council's initial "tumor board" assessment introduces an extra layer of subjective prioritization. Top public administration journals have cautioned that discretionary gatekeeping, even when expert-led, can suffer from inconsistent criteria or perceived favoritism when the decision process is not fully transparent. The FDA publishes limited details about voucher awards, but the pilot is still young; the broader community of policy observers will be watching for any signs that certain sponsors or therapeutic categories receive disproportionate benefit.
Long-Term Sustainability and Unanswered Questions
Several open questions persist: Can the agency sustain this pace without new appropriations? Will the initial seven approvals through May 2026 represent a steady state or an early anomaly? How will the FDA evaluate whether the pilot has actually improved domestic manufacturing or lowered drug prices, given that affordability is a stated priority? And if the program expands, what safeguards exist to prevent it from undermining the standard review pathway's integrity? These are not merely operational questions, they cut to the heart of regulatory design in public administration, where pilot programs must balance innovation with the responsibility to preserve public trust and scientific rigor over the long term.
Tropical disease priority review vouchers have sold for up to $290 million in a single transaction, with many deals landing between $100 million and $350 million. By making CNPV vouchers nontransferable, the FDA ensures that the accelerated review benefit stays with the product that earned it, rather than becoming a tradable asset.
Lessons for Designing Pilot Programs in Other Regulatory Contexts
What can other federal agencies learn from the FDA's Commissioner's National Priority Voucher Pilot Program? The CNPV pilot, launched in June 2025, offers a live case study in how to design a regulatory acceleration mechanism that balances speed, scientific integrity, and public purpose. For public administration careers charged with modernizing agency processes, four design features stand out.
Core Design Principles from the CNPV Pilot
Priority-based eligibility: The CNPV targets five explicit national health priorities: public health crisis response, innovative breakthrough therapies, large unmet medical needs, onshoring and supply chain resilience, and affordability. By linking eligibility to measurable policy goals, the program ensures that accelerated review serves a clear public interest rather than simply adding speed.
Collaborative review that preserves line authority: Applications undergo a multidisciplinary "tumor board-style" review by the CNPV Review Council, but final approval authority remains with the relevant FDA center. This model infuses cross-functional expertise into the decision process without diluting organizational accountability.
Nontransferable vouchers: Vouchers are granted to a specific drug or biologic application and cannot be sold or traded. This anti-commodification safeguard prevents a secondary market and keeps the focus on public health impact rather than financial arbitrage.
Unchanged statutory standards: All statutory and regulatory requirements for safety and effectiveness remain in place. The pilot compresses timelines, targeting review within 1-2 months versus 6+ months for standard priority review, without lowering the evidentiary bar.
Expedited Review Across Federal Agencies: Parallels and Lessons
While the FDA's voucher mechanism is unique, other federal agencies have experimented with accelerated pathways that share similar design elements. The Environmental Protection Agency's Efficient Producer Petition Process (EP3) expedites the review of certain fuel-pathway petitions under the Renewable Fuel Standard.1 EP3 prioritizes petitions that meet specific criteria, much like CNPV's priority-based eligibility, though it does not issue vouchers. Similarly, the Centers for Medicare & Medicaid Services' Transitional Coverage for Emerging Technologies (TCET) pathway accepts a limited number of emerging technologies and targets a national coverage determination within about six months of FDA market authorization.2 Both programs reflect a broader regulatory impulse to speed decision making for technologies with potential societal benefit, while retaining expert review and data requirements.
The Value of Structured Presubmission Engagement
One of the CNPV pilot's most exportable features is its presubmission phase, which facilitates structured early dialogue between sponsors and FDA staff. Before a formal application is filed, sponsors can clarify data expectations, address potential scientific concerns, and align on the evidence needed for a successful review. This reduces the risk of late-stage surprises and helps applicants prepare more complete submissions. For public administrators designing pilot programs in any regulatory domain, building in a comparable pre-application engagement window can lower barriers to entry and improve overall program efficiency.
What to Watch as the CNPV Pilot Evolves
As of May 2026, the CNPV pilot has yielded seven approvals, including a gene therapy for genetic hearing loss and a project strengthening domestic antibiotic manufacturing.2 Public administrators should monitor several developments: whether Congress considers codifying the pilot into permanent law, how the FDA publishes aggregated outcome data on review times and product safety, and whether similar voucher models expand to medical devices or other FDA-regulated products. The pilot's trajectory will offer critical evidence on whether a priority-voucher system can sustainably align regulatory acceleration with long-term public health returns.
Common Questions About the CNPV Pilot Program
The FDA's Commissioner's National Priority Voucher (CNPV) pilot program raises important questions for public administrators and policy professionals. Below, we address common inquiries about how the program works, its eligibility, and its implications.
What is the FDA Commissioner's National Priority Voucher pilot program?
The CNPV pilot program, launched in June 2025, is an FDA initiative that grants nontransferable priority review vouchers for drug or biological product applications addressing five national health priorities. It aims to accelerate regulatory review while maintaining all statutory safety and effectiveness standards, serving as a case study in regulatory innovation.
Can CNPV vouchers be transferred or sold to other companies?
No. Unlike other FDA priority review vouchers, CNPV vouchers are nontransferable. They are awarded by the FDA directly to sponsors for specific applications and cannot be sold or transferred. This ensures the program targets applications aligned with national health priorities without commercial voucher trading.
What affordability requirements apply to drugs approved under the CNPV program?
The CNPV program includes affordability as one of its five national health priorities. Products qualifying under this priority must demonstrate a meaningful impact on drug affordability, such as reducing costs for patients or the healthcare system. Specific affordability metrics or commitments are evaluated during the multidisciplinary review process.
How many products have been approved under the CNPV pilot program as of 2026?
As of May 8, 2026, the FDA has granted seven approvals under the CNPV pilot program. The first occurred on December 9, 2025, for a product strengthening domestic antibiotic manufacturing. Subsequent approvals include the first gene therapy for genetic hearing loss and a new molecular entity. Vouchers were awarded on December 19, 2025, and April 24, 2026.
How does the CNPV review process differ from standard FDA priority review?
The CNPV review targets times of 1-2 months, significantly faster than standard priority review of over six months. It uses a collaborative 'tumor board-style' review by a multidisciplinary CNPV Review Council, though final approval authority remains with the relevant FDA center. All safety and effectiveness standards are unchanged.
Is the CNPV pilot program permanent or does it require congressional authorization?
The CNPV program is a pilot initiative, not permanent. Launched under FDA's existing authority, its continuation or expansion may require further action or rulemaking. As a pilot, it tests the effectiveness of faster, priority-driven reviews aligned with national health priorities, and its future depends on evaluation outcomes and policy decisions.
Regulatory agencies today face growing pressure to deliver faster decisions without sacrificing scientific integrity, a tension that defines modern public administration. The CNPV pilot addresses this by pairing a cross-cutting review council with explicit national health priorities, compressing timelines to one to two months while preserving statutory safety and efficacy standards. For MPA and MPP professionals, the program offers a transferable blueprint: collaborative governance structures, priority-driven resource allocation, and rigorous evaluation can accelerate outcomes in any regulatory domain. Understanding what public policy is and how it shapes institutional design helps frame why the CNPV's architecture matters beyond drug regulation. Follow the pilot's evolving outcome data and its trajectory toward potential codification as a benchmark for designing the next generation of policy innovation.